ASTMH 2018, Aaron M. Samuels: “Antenatal clinic surveillance for malaria accurately reflects community malaria infection prevalence in a high transmission setting in western Kenya”
Collaborator(s): Centers for Disease Control and Prevention (CDC), United States
Countries: Ethiopia
Published: 29/10/2018
In collaboration with ASTMH, Image Audiovisuals, and session presenters, MESA brings you this webcast from the 67th ASTMH annual meeting in New Orleans, October 2018
Title: “Antenatal clinic surveillance for malaria accurately reflects community malaria infection prevalence in a high transmission setting in western Kenya “
Speaker: Aaron M. Samuels, Centers for Disease Control and Prevention-Kenya, Atlanta, GA, United States
Session information:
October 29, 2018, 10:15 AM – 12:00 PM, Marriott – Sheraton – Rodrigue Gallery (1st Floor)
Abstract:
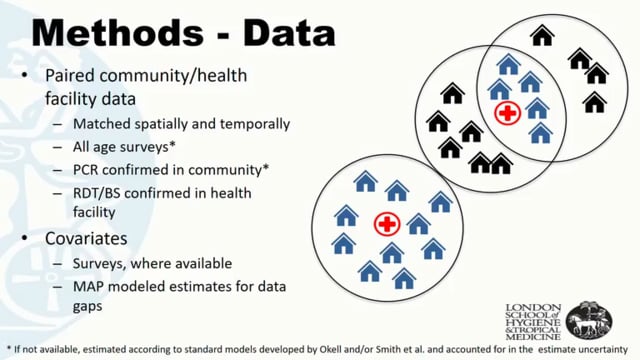
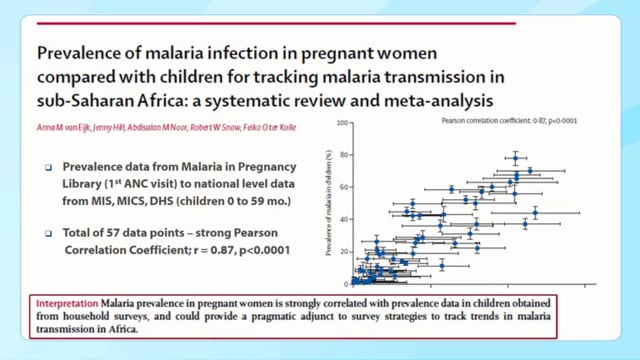
Surveillance systems in malaria endemic countries rely on passive detection of laboratory confirmed cases presenting to outpatient health facilities, community health workers, or other monitored outlets. In areas where many infections do not result in clinical symptoms, such as western Kenya where >75% of infections are asymptomatic, this strategy likely does not reflect community transmission dynamics. Community-based cross-sectional studies may provide more accurate estimates of infection, but are not scalable due to cost. Where antenatal care (ANC) attendance is high (>90% in western Kenya), pregnant women may serve as an easy access group as they are routinely screened for malaria during their first ANC visit. We compared 11 months of malaria prevalence data collected through a continuous community-based cross-sectional survey to test positivity rates in women attending first ANC visits collected from routine ANC records, to assess this population as a proxy for community malaria prevalence. Between April 2015 and June 2016 there were 998 first ANC booking visits with RDT results in the 5 health facilities, representing 10 geographic sub-locations. Of these, 110 (11.0%; 95% Confidence Interval [CI]: 9.2–13.1%) were RDT positive, with a test positivity rate range by sub-location of 2.5–20.3%, and by month of 3.8–15.5%. In the same geographic sub-locations over this period, 2108 individuals of all ages were tested for malaria by RDT in cMIS, and 436 (20.7%; 95% CI: 19.0–22.5%) were positive. Prevalence in cMIS by sub-location ranged from 12.3–39.5%, and by month from 8.5–28.4%. The Pearson correlation coefficient between ANC surveillance and cMIS by sub-location was 0.84 (p= 0.0098), and by time was 0.69 (p=0.025). We found a strong correlation between malaria RDT test positivity rate amongst women attending their first ANC booking visit and community malaria infection prevalence estimated by cMIS when comparing proportions over time and by geographic location. This suggests that in this area with a high first ANC coverage rate, pregnant women may present a sustainable proxy for trends in population malaria infection prevalence.
Published: 29/10/2018
THEMES: Surveillance | Vulnerable Populations
Related Resources