70th ASTMH Virtual Annual Meeting – 2021: Day 5
Sunday, 21st November 2021
Published: 24/11/2021

This report is brought to you by the MESA Correspondents Edima Ottoho, Tope Kayode, Franklin Tembongshu Formilack, Lucy W. Mwangi, Vita Mithi, Ana Alonso, Faith Hungwe, Olajoju Temidayo Soniran, Isabelle Delrieu, Patricia Doumbe Belisse, and Carlos A. Fernández Miñope. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri.
THEMES: THEMES: Basic Science | Epidemiology | Health Systems
MESA Correspondents bring you cutting-edge coverage from the virtual ASTMH 2021 Annual Meeting
Day 5: Sunday, 21st November 2021
S #119: Integrating Molecular Data into Malaria Surveillance: Progress in Senegal
Fatou Ba Fall (National Malaria Control Program – NMCP, Senegal) presented the progress and challenges toward integration of molecular epidemiology data into the decision making process by the NMCP. Senegal’s National Strategic Plan 2021-2025 aims to reduce transmission by at least 75%. Through epidemiological profile analysis, 3 zones were selected and stratified by transmission level. Surveillance was conducted to follow the evolution of the disease in time. Since 2001, malaria mortality and morbidity has reduced by ~30%, reaching 3.81% proportional morbidity in 2020. Low levels are now an issue and hard to manage by malaria surveillance. Senegal aims now to eliminate malaria by 2030. Genomic data can have an important role in surveillance, allowing to reorient and better select interventions and priorities. This included the genetic surveillance of drug resistance markers (PfCRT-76T, PfMDR-86Y, PfMDRTT-184F) of importance for the first line of antimalarial treatment. Genetic information helped to differentiate between local and imported infections; also, revealed transmission patterns. Ba Fall stated at the end that in fact, this information has been used in the decision making by NMCP.
July Thwing (Centers for Disease Control and Prevention – CDC, United States of America) in her talk developed diverse ways to design sampling strategies in health facilities and community levels. At health posts, blood samples and positive rapid diagnostic tests (RDTs) samples were collected in sites of interest to the National Malaria Control Program of Senegal. At community level, she reported that sampling was performed in three sites Sessene, Ndoga Babacar and Kedougou. Besides, a cross sectional survey was performed in schools and a proactive model in which community health workers (CHWs) visited all households, known as PECADOM plus platform “Prise en charge du paludisme à domicile”, was deployed. Thwing emphasized the importance of this system and the opportunity to use it as a surveillance tool to measure impact. PECADOM mainly focused on household weekly visits to identify fever cases, offer RDTs and treat positives, and on the other hand on the collection of filter paper samples and basic demographic data. She highlighted at the end that those sampling frameworks help them to get malaria transmission dynamics, seasonal transitions and population seroprevalence, important metrics for basic surveillance.
Aida Badiane (University Cheikh Anta Diop, Senegal) talked about epidemiological measures of infectious disease with a great focus on serosurveillance through multiplex serology. She started by explaining the interests of epidemiological measures, they are the foundation to monitor diseases, formulate and evaluate healthcare policy, and conduct scientific research. She deeply explained the importance of serosurveillance in the detection of malaria exposure over time to understand disease burden and to measure change when malaria incidence and prevalence are low. Badiane talked about a relevant advantage of serosurveillance through multiplex serology, which can detect and quantify dozens of antigens simultaneously. Then, she also presented some ways to implement serosurveillance like community-based cross sectional surveys or a survey in a sentinel site. She also reported results from a survey performed in 24 sentinel sites by the NMCP of Senegal. Results show two types of antibodies PfMSP-1 and LSA-1 which could be categorised by age group and area. She concluded by stating some things to be considered for sustainability of serosurveillance like maintenance of skills, maintenance of equipment and procurement of reagents.
At the onset of her talk, Caitlin Bever (Institute for Disease Modeling – IDMOD, United States of America) presented different models to show that models help to take information available and turn it into actionable information. It helps to unify the framework for understanding diverse field observations. Bever then reflected that a very relevant and well-known country-led approach to malaria program decision-making known as high burden to high impact (HBHI) is supported by different models that assess different data. She also highlighted that there is a need to assess the constant impact of interventions and also the role of malaria imported cases in sustaining malaria transmission in different regions. Bever reminded the attendees that to use models, we have to define data of interest and types of data in advance and that a model informs you of how to collect efficient and informative data in programmatic mode.
S # 125: Dihydroartemisinin-piperaquine as an Alternative Drug for Intermittent Preventive Treatment for the Control of Malaria in Pregnancy in Areas of High Sulphadoxine-Pyrimethamine Resistance in East and Southern Africa
WHO recommends intermittent preventive treatment (IPTp) with sulphadoxine-pyrimethamine (SP) for preventing malaria in pregnancy, but high-level SP resistance threatens its efficacy in parts of East and Southern Africa. Mwayiwawo Madanitsa (University of Malawi, Malawi) presented the findings of a randomized trial that compared the efficacy of IPTp with sulphadoxine-pyrimethamine (SP) versus dihydroartemisinin-piperaquine (DP) with or without azithromycin (AZ) in reducing adverse pregnancy outcomes in Kenya, Malawi & Tanzania. He commenced by reporting alternative prevention strategies tested (between 2007 and 2019) amongst which only DP was promising compared to SP. Madanitsa’s study was a multi-center, 3- arm (monthly SP, monthly DP, and monthly DP + AZ), a parallel trial conducted from 2018 to 2021. 4680 women were enrolled, administered a monthly treatment, and followed up to 8 weeks postpartum. Both DP arms performed worse than SP at preventing adverse pregnancy outcomes. The beneficial effects of SP were driven by better fetal growth resulting in fewer low birth weight newborns. There was no difference in preterm delivery, fetal loss, and neonatal death across all arms. DP significantly reduced malaria relative to SP. He recommended that DP should not replace SP as IPTp even in areas with high SP resistance.
Feiko ter Kuile (Liverpool School of Tropical Medicine, United Kingdom) presented a meta-analysis that compared intermittent preventive treatment (IPTp) with dihydroartemisinin-piperaquine (DP) versus sulphadoxine-pyrimethamine (SP) for the prevention of malaria in pregnancy and adverse pregnancy outcomes in Kenya, Malawi, Tanzania, and Uganda. The study aimed to provide definitive evidence for WHO’s policymaking. Eight data sets (with a combined 6687 pregnancies) were pooled from six trials. The 6687 pregnancies were separated into two arms – DP and SP – based on the IPTp taken. Clinical malaria, placental malaria, and malaria at delivery were lower in the DP arm. DP was not superior to SP in preventing adverse pregnancy outcomes (fetal loss, low birthweight, preterm delivery, neonatal death) in the different gravidae groups. However, small for gestational age was less frequent in the SP arm and birthweight-for-gestational age z-scores were higher in the SP arm. Birthweight was 49g higher in the SP arm, possibly reflecting better gestational weight gain (GWG) per week in this arm. Dr. Ter Kuile suggested that future studies should explore the antimalarial activity of DP and the non-malarial effects of SP in a DP + SP combination.
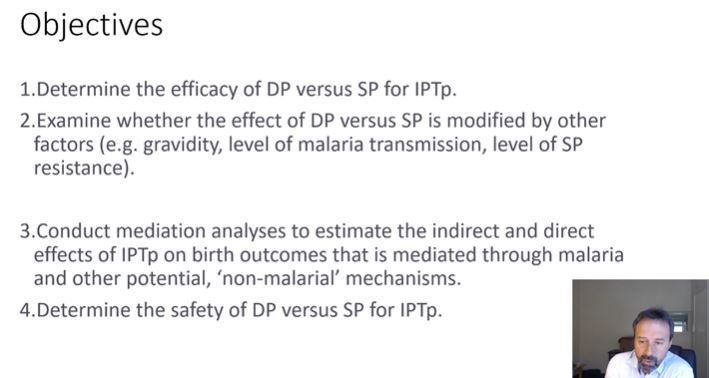
The study presented by Michelle Roh (University of California San Francisco (UCSF), United States of America) aimed to break down the antimalarial and non-malarial effects of IPTp drugs on birth weight, and to quantify the effect of Sulphadoxine-Pyrimethamine (SP) on gestational weight gain (GWG) contributing towards birth weight. Mediation analysis is an epidemiological method that quantifies the extent to which an intermediate variable influences the effect of an exposure on an outcome. Roh and her team conducted mediation analyses using data from 6603 pregnant women included in a meta-analysis resulting in live births. Her results showed that despite its greater effect on malaria prevention, DP appears to only have a slightly greater antimalarial benefit on birthweight, though this effect may vary by malaria transmission setting. Consistent with Roh’s previous mediation analyses of 3 studies, SP appears to exhibit non-malarial benefits on birth weight, and this may be due, in part, to SP’s greater effect on GWG. Sensitivity analyses will be conducted to rule out bias due to potential unmeasured confounding and mismeasurement of the mediator. Furthermore, more sophisticated mediation analyses will allow assessment of the independent contribution of factors in mediating the SP and birth outcome pathway, using longitudinal measurements of malaria and gestational weight gain. Future studies will focus on assessing effect modifiers that may explain the heterogeneity in the overall and mediated effects.
Concerns about Sulphadoxine-Pyrimethamine (SP) resistance have led to trials exploring repeated treatment courses of dihydroartemisinin-piperaquine (DP) as an alternative for malaria chemoprevention. However, piperaquine is associated with dose-dependent prolongation of the cardiac QT interval that may lead to increased risk of serious arrhythmia and Torsades de Pointes. Julie Gutman (Centers for Disease Control and Prevention, United States of America), presented an individual participant data meta-analysis on the cardiotoxicity of dihydroartemisinin-piperaquine (DP) when used for IPTp for the prevention of malaria in pregnancy. Repeated doses of DP were found to be safe. Study specific correction of the QT provided the best adjustment for heart rate. Prolongation of the QT interval greater than 480 ms was infrequent and prolongation greater than 500 ms was rare. Corrected QT (QTc) prolongation occurred most frequently after the initial course, with fewer individuals exhibiting extreme QTc prolongation with subsequent courses, suggesting a tolerance mechanism, and highlighting that repeater courses are not associated with an increased risk for QTc prolongation.
S #130: Expanding the Use of Safe and Effective Radical Cure of Relapsing Malaria: Defining Populations at Risk of Hemolysis
Ari Winasti Satyagraha (Eijkman Institute for Molecular Biology, Indonesia) spoke about glucose-6-phosphate dehydrogenase (G6PD), an X-linked gene known for its antioxidant activity in erythrocytes. G6PD deficient individuals may develop acute haemolytic anaemia when exposed to oxidative malarial drugs like primaquine/tafenoquine. G6PD phenotypic expression in females is varied (low: <30% of normal activity, usually calculated as the Adjusted Male Median; intermediate: 30-70% of AMM; normal: >70%of AMM). In this study, Satyagraha’s aim was to determine the degree of haemolysis in the intermediate female G6PD activity cohort who are capable of haemolysing. In another study, they evaluated malondialdehyde (MDA) and glutathione (GSH) levels to determine the extent of membrane damage caused by oxidative stress. A Carestart Biosensor quantitative assay was conducted and it was found that most females who were primarily infected with Plasmodium falciparum (Pf) were located in the middle of the histogram. These results enabled Satyagraha to determine the population’s minimum G6PD activity threshold for counteracting oxidative stress, that is, females who are capable of undergoing primaquine/tafenoquine therapy. MDA and GSH results showed that higher G6PD activity does provide increased protection against oxidation. More MDA and GSH work still needs to be conducted on intermediate G6PD activity female cohorts to better understand the pharmacokinetics.
Benedikt Ley (Menzies School of Health Research and Charles Darwin University, Australia) spoke of how 8-aminoquinolines drugs effectively remove hypnozoites from the liver but are not often prescribed because they cause severe drug induced haemolysis in G6PD deficient (G6PDd) patients. The aim of this study was to assess whether G6PD activity increased during plasmodium infection. They used study results from studies conducted in Bangladesh in the last seven years. Ley compared G6PD activity between a treatment efficacy survey (G6PD participants with malaria) and a cross-sectional survey (G6PD participants with no malaria). In addition, they conducted a case control study that enrolled G6PDd participants (with no history of malaria versus history of malaria) to quantify the potential protective effect of G6PD deficiency against malaria which would affect the outcome of the former comparison. The clinical trial aimed at evaluating the efficacy of national treatment guidelines whilst the cross-sectional survey assessed G6PDd prevalence in the local population. A mixed method approach was used and found that G6PD activity significantly differed between participants with and without malaria infection. However, no significant difference between aparasitemic and sub-microscopic participants was observed but Ley believed that had a clinical relevance. He concluded his talk by stating the limitations of the study that it did not factor G6PD activity change over time. This could be rectified in a more incorporative longitudinal study.
James Watson (Mahidol Oxford Tropical Medicine Research Unit, Bangkok) talk was on determinants of hemolysis following primaquine administration in G6PD deficiency. He pointed out that hemolysis in G6PD deficiency is determined by multiple factors; dose of primaquine, exposure to the primaquine metabolites, G6PD mutation, disease effect in malaria vs. healthy volunteers and red cell age distribution. Watson outlined that G6PD deficiency reflects an unstable enzyme that has the tendency of degrading rapidly; functional enzyme activity in reticulocytes is higher than in mature erythrocytes, and older cells hemolyze first. The presentation focused on the age distribution of the red cells in individuals given primaquine and how this determines the existence of hemolysis in a clinical trial using data of healthy volunteers that were G6PD deficient, in ascending primaquine dosing of healthy males. Participants were given regimes between 15 and 20 days with the smallest dosing of 7.5mg and the largest dosing of 45mg. They recorded daily hemoglobin, and applied rules on safety and monitoring of clinical symptoms of participants throughout the trial. In the second half of the trial, a total dose of 5-8 mg/kg was given for 15 days. The results showed a 25% – 33% decrease in hemoglobin. However, dose escalation was stopped in 1 symptomatic person because there was more than 30% drop. Decline in hemoglobin was dependent on the rate of primaquine escalation and hemoglobin initiation. However, for P. vivax malaria, the hemolysis is seen after admission and following treatment is due to disease and not the drug. In conclusion, the degree of hemolysis in G6PD deficiency is dependent on red cell age distribution.
Cindy Chu (Shoklo Malaria Research Unit, Thailand) presented the overview of data to date on clinical hemolysis caused by 8-aminquinoline. She emphasized the degree of clinical haemolysis and associated phenotypes in addition to the G6PD activity phenotype. Early research done in the 1950-70s focused on the clinical aspect of hemoglobin drops, and dose dependent primaquine related hemolysis. These early trials also observed that hemolysis was most common in some adversities. In the 1970-80s, focus shifted to the characterisation of the G6PD genotype and phenotype. Today the genetic data has not been analyzed together with the G6PD phenotype or clinical hemolysis, and it is even rare to combine all three aspects. This forms a research gap that needs to be breached. Chu urged clinicians to pay more attention to haemoglobin recovery and advocating for a revised version of the WHO classification of mutation based on risk assessment of clinical haemolysis. The revised classification will assist in providing more accurate clinical data. Chu concluded her talk by reiterating the importance of conducting work aimed at reclassifying haemolytic drugs whilst considering the factors involved in haemolysis and haemolysis recovery.
S #136: Implementing Malaria Chemoprevention Campaigns During the COVID-19 Pandemic
Abimbola Phillips (Malaria Consortium – MC, Nigeria) started his talk by explaining that MC provided community distributors (CDs) to deliver seasonal malaria chemoprevention (SMC) door-to-door in the midst of COVID-19 pandemic increasing the risk of infection. Then they conducted a cross-sectional study in Kano and Sokoto States to assess CDs’ adherence to the infection prevention control (IPC) guidelines developed by MC. Findings showed a greater availability of IPC equipment for SMC in Sokoto than in Kano. For adherence to IPC practices, in Kano, practice of hand hygiene for at least 30 seconds occurred at only 0.7% of 1503 possible opportunities, while in Sokoto, it occurred at 3.6% of 1578 possible opportunities. There was no disinfection of sulfadoxine-pyrimethamine (SP) together with amodiaquine (AQ) blisters, nor safe disposal of masks/wipes at any instance in Kano, but in Sokoto. Masks were used 62% of possible times in Kano, but 74% in Sokoto. CDs maintained safe distancing at 5.1% of times in Kano but 16% in Sokoto. Adherence variance among CDs, influenced by equipment availability, training on procedures, community members’ reactions and difficulty in keeping appropriate physical distance. Adequate knowledge, CDs’ positive perceptions of the IPC measures and feasibility of implementation were adherence drivers.
Assane Kano (Catholic Relief Services – CRS, Niger) presented a study on the integration of SMC and malnutrition screening in Niger, prior to and during the COVID-19 pandemic based on an analysis of routine data collected since 2016. He explained that CRS is a principal recipient of a 3-year Global Fund project, with the goal of 40% malaria morbidity and mortality reduction in 8 regions and 72 health districts, and one of its key interventions is SMC. He explained that SMC has evolved over the years from 12-17 health districts coverage and stand-alone campaigns in 2013-2015 to 28-61 health districts, and integrated campaigns in 2016-2021, with increased partners’ funding/support. Also, a door-to-door approach was adopted over the previous fixed sites SMC and malnutrition campaign approach since COVID-19 hit Niger in March, 2020, resulting in an increase in SMC annual target from 205,959 to 4,289,520; and coverage from 86% to 105% from 2016 to 2020 respectively. Similarly, malnutrition intervention, since its integration with SMC, has improved annual coverage from 54% in 2016 to 109% in 2020 because Community distributors now reach more targeted children in their homes.
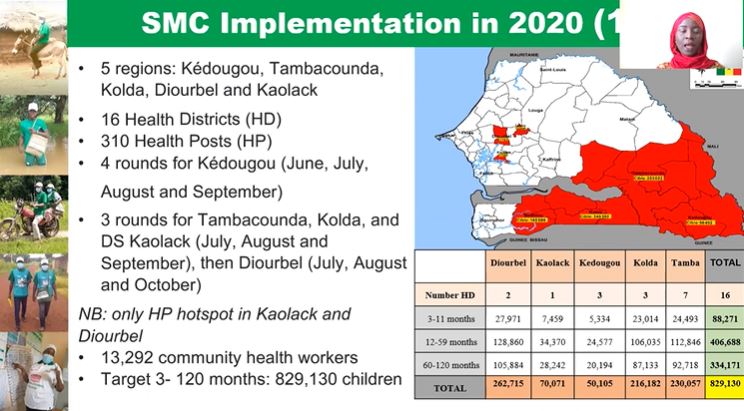
Seynabou Gaye (National Malaria Control Program – NMCP, Senegal) presented findings from a study titled, ‘Implementing Directly Observed Treatments for Three days (DOTS3) for SMC during the COVID-19 pandemic in Senegal’. They implemented SMC in 5 regions in Senegal, adopted a mass campaign approach, used community volunteers and administered 3 to 4 treatment passages of SP + AQ at monthly intervals. There was a theoretical coverage of 85.8% of children aged 3-120 months, of which 96.3% received the 3rd dose of CPS. There was an overall achievement of SMC goals, stakeholders were trained and developed a memorandum on the prevention rules COVID-19 during the SMC campaign. They made sure to warn of side effects early using the 3-day direct observational treatment (DOT) approach. In the end, Gaye stated how crucial was the support and involvement of partners in the implementation, including health committees and local authorities.
Pedro Aide (Manhica Health Research Center – CISM, Mozambique) presented results from a malaria mass drug administration (MDA) amongst displaced populations in the province of Cabo Delgado in Mozambique. The objective of the MDA was to reduce the burden on health services through the reduction in malaria transmission, morbidity and mortality, even though public health had been weakened by population growth resulting from migration to relatively safe regions. For all the eligible population, 3 rounds of MDA were given, aiming to cover the entire malaria transmission season: february, april until the end of May. They used a door-to-door implementation strategy and a scanning strategy to reach most households in the village before moving on to the next village. They found the need for a strategy of triangulating data from different sources before the start of each round including information from village leads about population movements. More support staff was needed beyond district personnel, both in terms of fieldworkers and coordinators. Aide concluded by highlighting some key messages MDA was successfully delivered in a challenging environment, coverage was improved between the different rounds of MDA, campaigns managed to avoid an expected increase in malaria cases, and both communities and internally displaced people (IDP) camps benefited from the campaign.
S #140: Eliminating Malaria in the Guiana Shield During COVID-19 Times: How Can We Accelerate It?
Introductory remarks by Leopoldo Villegas (ASOCIS, Venezuela) outlined the uniqueness of the Guiana Shield. Geographically, the Guiana Shield underlies Venezuela, Guyana, Suriname and French Guiana as well as parts of Colombia and Brazil and is home to numerous minerals, majorly gold. This region, he went on to explain, is responsible for most of the malaria transmission in South America, mainly due to malaria importation from the mining areas to the hinterland; as well as some of the most multi-drug resistant malaria parasites. Nonetheless, Villegas noted that there have been significant strides in malaria in the region especially over the last decade as there has been concerted efforts made in countries on both extremes of the malaria spectrum that is the malaria-free to high transmission areas; however mobile and hard-to-reach populations remain the most important and affected groups.
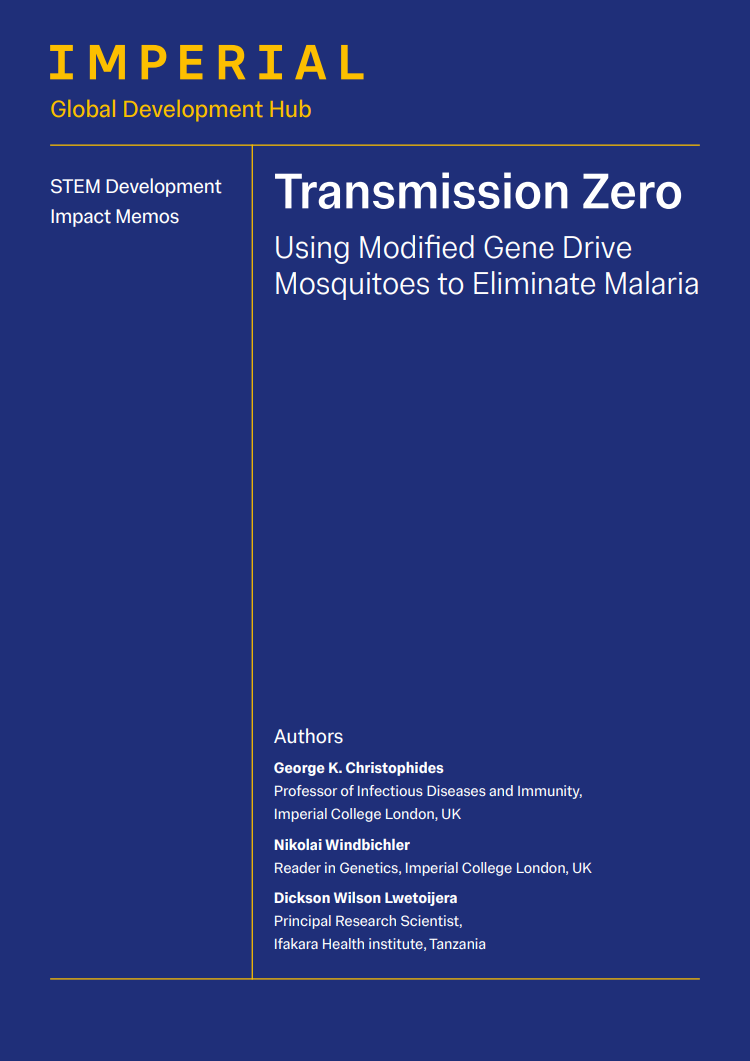
Guyana, a country with about 750,000 inhabitants with limited access to care, sees about 20,000 cases of malaria per year, majority caused by P. vivax (Pv), some by P. falciparum (Pf) and a little by P. malariae. In 2020, 76% of the infections in the hinterland were due to migration to areas of gold mining and logging for economic benefit. Then Horace Cox (Ministry of Health, Guyana) discussed the lessons from malaria diagnosis, treatment and elimination in sentinel sites. Therapeutic efficacy studies (TES) in 2014 revealed Pf K13 mutations indicating parasite resistance to artemether-lumefantrine (AL); while in 2019 AL was found an efficacious treatment and no mutations were detected. Though microscopy was the standard mode for routine malaria diagnosis, rapid diagnostic tests (RDTs) were used to supplement testing while polymerase chain reaction (PCR) was employed in this study. Interestingly, Cox observed an increase in slide positivity rate, yet the number of tests done decreased. He emphasised that innovation is needed to accelerate testing, ensure universal access to diagnosis and treatment, and expand surveillance. Further, the relationship between human behaviour, risk perception and knowledge was assessed observing that risk did not drive human behaviour, and knowledge influenced behaviour more than perception. Aside from migration to mining camps, other factors contributed to malaria transmission, including seasonality and the price of gold. With respect to mosquito capture methods, the Shannon modified trap was found to be the best. In addition, Cox stated the importance of studying parasite genetics for a better understanding of mutations, host-parasite interactions and therapeutic efficacy. In conclusion, Cox outlined four pillars for malaria elimination learned through their study as: (i) ensuring universal access to vector control; (ii) ensuring universal access to case management; (iii) transforming surveillance systems and (iv) collaboration to create tailored interventions and illustrative as well as educational materials for malaria prevention.
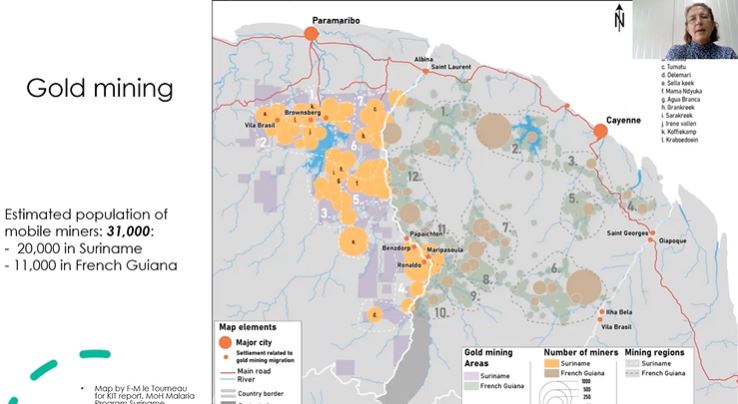
Lise Musset (Institut Pasteur de la Guyana, French Guiana) started her presentation with a descriptive narrative on geographical location of French Guiana, population, shared context with neighboring countries and its impact on malaria transmission. In the past decade, malaria cases caused by P. falciparum and P. vivax reduced greatly but Pv cases increased slightly in 2016. Interestingly, she noted that no malaria mortality was recorded since 2013, but in 2020 only 4 cases of Pf malaria were recorded out of which 2 were imported cases. Musset stated that these results were achieved due to implementation of interventions which included new drugs and accelerated deployment of rapid diagnostic tests from 2007 to 2010; community approach in neighboring countries in 2009; some operational research programs on better malaria control conducted between 2015 and 2019; and military operation against illegal gold mining. One of the programs implemented was the Resistance and Emergence to Artemisinin and its partner drugs in the Guiana Shield to Identify them to better Restrain (REAGIR), whose findings showed that artemether-lumefantrine was still efficacious, and identified two malaria transmission hotspots. Another was PALUSTOP which employed active case detection by PCR followed by systematic treatment of positive cases. Musset also emphasised the importance of collaboration through which the MALAKIT project was implemented. In the end, she highlighted main drivers for malaria transmission as (i) living in a remote area close to the forest, (ii) occupational activities such as gold mining, agriculture and hunting, (iii) having poor knowledge regarding malaria, and (iv) Pv transmission.
Helene Hiwat (Ministry of Health, Suriname) commenced with a brief description of the Republic of Suriname, noting that in the coast there is no malaria but in the interior region malaria transmission is still taking place. She briefly highlighted the history of malaria in Suriname stating the changing malaria epidemiology due to mining activities and cross-border movement of gold mining populations from French Guiana. Hiwat noted that since 2018 low malaria incidence was observed in the country with some re-introduction of Pv malaria, but these outbreaks had been contained since August 2021. Unfortunately, re-introduction of P. vivax had been reported due to cross-border movement of gold mining populations. Hiwat outlined primary malaria interventions as targeted outreach and health education to at risk populations; improved provision of malaria services; border screening posts; provision of Malakit for self-diagnosis and self-treatment; mass distribution of long lasting insecticide-treated nets (LLINs) among high risk populations; and implementation of National Malaria Elimination plan 2021-2025. She concluded by enumerating important lessons from malaria elimination efforts in Suriname as (i) engaging at-risk populations, (ii) lowering barriers, (iii) remind health workers about malaria through continuous training (iv) integration of malaria programs within existing public health programs, (v) innovation, (vi) in country and cross-border communication and collaboration.
This report is brought to you by the MESA Correspondents. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri (Lindsley F. Kimball Research Institute, New York Blood Center, USA). This report is cross-posted on the MESA website and on MalariaWorld.
Published: 24/11/2021
This report is brought to you by the MESA Correspondents Edima Ottoho, Tope Kayode, Franklin Tembongshu Formilack, Lucy W. Mwangi, Vita Mithi, Ana Alonso, Faith Hungwe, Olajoju Temidayo Soniran, Isabelle Delrieu, Patricia Doumbe Belisse, and Carlos A. Fernández Miñope. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri.
THEMES: Basic Science | Epidemiology | Health Systems
Related Resources