70th ASTMH Virtual Annual Meeting – 2021: Day 3
Friday, 19th November 2021
Published: 22/11/2021

This report is brought to you by the MESA Correspondents Edima Ottoho, Tope Kayode, Franklin Tembongshu Formilack, Lucy W. Mwangi, Vita Mithi, Ana Alonso, Faith Hungwe, Olajoju Temidayo Soniran, Isabelle Delrieu, Patricia Doumbe Belisse, and Carlos A. Fernández Miñope. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri.
THEMES: THEMES: Basic Science | Epidemiology | Health Systems
MESA Correspondents bring you cutting-edge coverage from the virtual ASTMH 2021 Annual Meeting
Day 3: Friday, 19th November 2021
Symposium #52: Trials of Malaria Vaccines in Pregnant Women
Blair Wylie (Beth Israel Deaconess Medical Center, United States of America) started her presentation with a keen look at the impact of COVID19 in pregnancy which has a higher risk of complications and death among pregnant individuals. Even though preliminary data on mRNA vaccines in pregnancy showed a very similar side effect profile to that in the general population, vaccine coverage in pregnancy in the USA is still very low < 30%. This can be attributed to a number of reasons. Pregnant women have historically been excluded from participation in clinical trials, after some drug interventions famously caused harmful sequelae during pregnancy ex. thalidomide and diethylstilbestrol. However, when women are excluded from trials, safety data must then be gathered post-licensure during routine use rather than from randomized control trials, leaving the perception that vaccination during pregnancy may be unsafe, and consequently putting more women at risk of harm. Wylie then pivoted to malaria vaccines during pregnancy, an ideal indication for vaccination especially with the heavy burden of adverse outcomes associated with maternal malaria for the mother and the fetus. She concluded by emphasizing that complications occur in pregnancy and these vary by gestational age, therefore these baseline complication rates need to be taken into consideration when designing a clinical trial in pregnancy so as to not over-ascribe harm to the intervention (e.g., vaccine).
Michal Fried (National Institute of Allergy and Infectious Diseases – NIAID, United States of America) described the role of a pregnancy registry to prepare for a vaccine trial in pregnant women. She first described a longitudinal cohort study in Ouelessebougou, Mali, that highlights the urgent need for a malaria vaccine for pregnant women: of the 1850 women enrolled, about 70% of women harbored the malaria parasite at least once during the pregnancy with the majority diagnosed at enrolment. Malaria infection during pregnancy increased the risk of stillbirth and preterm delivery in primigravidae and the risk of early neonatal death in multigravidae. Subsequently, a pregnancy registry study was conducted to collect baseline information on pregnancy outcomes and involved two cohorts. In the first cohort enrolled during antenatal clinic visits (ANC), the largest proportion of the 1814 pregnant women enrolled were aged 20-35 years, multigravid, used insecticide treated nets (ITNs), received 1-2 courses of intermittent presumptive treatment in pregnancy using sulfadoxine-pyrimethamine (IPTp-SP), and first attended ANC during their second trimester. Maternal factors associated with perinatal death were primigravida and age <20 years. Odds of low birth weight (LBW) were higher in primigravidae and women aged <20 years. In the second cohort of women of childbearing age who were enrolled before conception, 799 non-pregnant women were followed for 2 years to observe early pregnancy and its outcome. Preliminary data analysis of 357 pregnancies revealed that the largest proportion of women were multigravidae aged 20-25 years; miscarriage was the most common adverse outcome. Primigravidity and malaria infection were independently associated with preterm deliveries. This background information on poor pregnancy outcomes and risk factors is the key to design and monitor future interventional trials in pregnant women.
Halimatou Diawara (University of Sciences, Techniques and Technologies of Bamako – USTTB, Mali) began her talk by reiterating that malaria is indeed a huge public health challenge especially among pregnant women; statistics show that about 11 million pregnant women in sub-Saharan Africa are infected with malaria annually. She further emphasized that there is an urgent need for new tools to control malaria during pregnancy. Diawara went on to describe trials conducted in Ouelessebougou, Mali, using Sanaria, Inc. PfSPZ Vaccine candidate, in order to prepare for future trials in pregnant women. PfSPZ has previously been found to be efficacious for preventing infection in healthy malaria-exposed adults. The group observed that a short 4-week PfSPZ Vaccine regimen is safe among women of childbearing potential (WOCBP) and confers significant efficacy against Plasmodium falciparum infection and, for the first time, against clinical malaria episodes. Also for the first time, the team observed that the efficacy of PfSPZ Vaccine persisted for two years, against both P. falciparum infection and clinical malaria. The team concluded that the short 4-week vaccine regimen will be appropriate to test in pregnant women and that presumptive antimalarial treatment before immunization seems to be a requirement for PfSPZ Vaccine field efficacy.
Morten Nielsen (University of Copenhagen, Denmark) discussed his ongoing work to optimize vaccines based on the VAR2CSA protein that the parasite uses to bind and sequester in the human placenta. He suggested that the target product profile of the vaccine would require two doses, could be administered prior to pregnancy, and would target the majority of VAR2CSA genotypes. In phase 1a/b trials, two VAR2CSA vaccine candidates (PAMVAC and PRIMVAC) were safe and well tolerated, immunogenic, generated antibodies reacting with homologous VAR2CSA-expressing parasites, and induced functionally active antibodies. Further studies are ongoing to determine the longevity of the immune response, the capacity to be boosted by natural exposure, and cross-reactivity of vaccine-induced immune responses. His team is now analysing CLP-based PAMVAC and multi-PAMVAC nanoparticle vaccines. The platform used for the vaccine is simple, versatile and universal to create capsid virus-like particles (cVLP) for any antigen. Lessons from the recent scale up of the COVID-19 vaccine as well as the vaccine against human papillomavirus supports the manufacturability of such cVLP-based vaccines. Nielsen concluded that novel vaccines or novel modes of administration of vaccines are needed for malaria vaccine development; and that a combination of vaccines targeting different parasite stages may lead to greater efficacy.
Symposium #57: Alan J. Magill Malaria Eradication – Keeping Malaria Eliminations on Track (The Successes and Challenges on the Pathway to Eradication)
The symposium began by paying tribute to Alan J. Magill, the former ASTMH president and congratulating Tshokey Tschokey (Bhutan); the 5th Magill Fellow (2021).
María Eugenia Grillet (Central University of Venezuela, Venezuela) started her presentation with an overview of malaria morbidity and mortality in the Americas during the past decade, and the major cause of malaria being Plasmodium vivax (76%) followed by Plasmodium falciparum (24%). She mentioned examples of E-2020 countries that are certified malaria-free and lessons that can be learned from them which includes political commitment, strong surveillance system, prompt diagnosis, appropriate treatment, adequate preventive, control measures, and adequate funding. Over the past decade, nine countries have experienced an increase in malaria cases but this is more noticeable in Venezuela. She identified some of the challenges limiting progress of the malaria elimination agenda in Venezuela as political instability and socioeconomic collapse which has increased cross-border malaria transmission in neighboring countries; high biodiversity and distinct feeding behavior of the mosquitoes enhances transmission of the disease; deforestation and illegal mining increases mosquito breeding sites; limited diagnostic methods; antimalarial drug policy and outbreak of COVID-19 epidemic. She concluded by reiterating key gaps that need immediate attention and recommendations for elimination of malaria in the Americas.
Rajesh Panjabi (President’s Malaria Initiative – PMI, United States of America) congratulated those involved in the RTS,S/AS01 malaria vaccine production; a significant milestone towards malaria elimination. Panjabi advocated for the continued use of the vaccine with other malaria control tools. He then enumerated the challenges facing malaria eradication: insufficient coverage, increasing costs and insufficient funding, setbacks caused by the COVID-19 pandemic, constant changes in vector and parasites, civil conflicts that hamper elimination strategies and climate crises. However, success in reducing mortality rates has been achieved in 22 PMI countries within Africa. PMI has partnered with sub-Saharan African countries in order to address malaria-based challenges. They have adopted a subnational approach to elimination that is being used to ultimately reach national elimination. Panjabi outlined PMI’s focus areas as reaching the unreached; strengthening community health systems; keeping malaria services resilient against current and emerging threats; innovating and leading by leveraging new tools and shaping global priorities to end malaria faster, and investing locally. In conclusion, he acknowledged the efforts of the Africa CDC and challenged us to relentlessly pursue malaria elimination so as not to succumb to the ideology and satisfaction of malaria control.
Corine Karema (National Malaria Control Program – NMCP, Rwanda) began her talk by firstly, reminding us why malaria eradication matters and secondly, telling us about the efforts Rwanda has made to reduce its malaria incidence rates. Rwanda’s malaria reduction is attributed to the combined effective use of innovative and transformative tools as well as applying lessons learnt from the COVID-19 pandemic. Karema mentioned that deploying the right prevention tools at the right time to the right places is fundamental to malaria elimination, especially in high-burden countries. This is possible by improving program management, designing strong and sustainable systems and empowering local capacity for efficacious implementation and service delivery. The COVID-19 pandemic emphasised these approaches as countries that valued and invested in strong governance, strategic monitoring, health systems and frontline workers were better positioned to mitigate risks and losses. This is a challenge in Africa where most healthcare systems are fragmented, consequently, disease preparedness and monitoring is fragile thus recovery from severe disease outbreaks is gradual. Currently, many opportunities paving the way for malaria eradication exist and Karema believes that these tools will make it possible to end malaria in a generation.
Pedro Alonso (WHO Global Malaria Programme, Switzerland) began his presentation by applauding the efforts made by China towards malaria eradication. It was from this that Alonso wanted to draw out elements that can aid in achieving malaria eradication. He then defined malaria elimination and stated how the number of countries that are achieving certification continues growing. Certification requires that a country fulfils the strict eradication criteria and evaluation process which includes having no indigenous malaria cases for three years. China, once a malaria endemic country, was able to achieve this phenomenon. It focused on a comprehensive disease prevention and control system, stratified effective implementation strategies and invested in its socio-economic development. From their efforts, Alonso highlighted six principles of elimination that China used and five lessons learnt from countries that have already eradicated malaria. The key element mentioned was adopting a ‘Whatever it takes!’ attitude. Alonso concluded his motivating presentation with a quote from Boyd (1939), “Malaria control should not be a campaign, it should be a policy, a long term program. It cannot be accomplished by spasmodic effort. It requires the adoption of a practicable program, the reasonable continuity of which will be sustained for a long term of years.“
Symposium #60: Malaria: Data to Inform and Target Malaria Elimination Strategies
Rodrigo M. Corder (University of Sao Paulo, Brazil) presented work on the contribution of low-density and asymptomatic infections to Plasmodium vivax transmission in the Amazon. The main question Corder tried to answer was: “What is the relative contribution of sub patent and asymptomatic infections to P. vivax transmission in the Amazon?” Results showed that 60.7% of PCR-diagnosed infections were missed by microscopy and 70.9% were asymptomatic in 34 population-based surveys across the region. The top 20% spreaders in the 4 sites, two in Peru and two in Brazil, were estimated to contribute between 78.8% and 92.9% of all P. vivax transmission events in each site. By estimating the relative contribution of low-density and asymptomatic infections to P. vivax transmission in the Amazon, they inferred that subpatent parasite carriers contribute little to the overall transmission in their study population. Potential implications for malaria elimination strategies in this region are understanding that conventional microscopies may suffice to identify the vast majority of infections that contribute to human-to-mosquito transmission of P. vivax and that ultra-sensitive molecular techniques may not be a fundamental component of malaria elimination programs in the region.
Prayuth Sudathin (University of Public Health, Thailand), began his presentation on using source of infection data to target malaria elimination in Thailand by highlighting the background of malaria elimination strategy surveillance and response approach which prioritise evidence-based employment in the country. The study adopted the routine data of 2016-20, which was used to assess whether associations increase infections and understand validity in identifying remaining hotspots. Data of interest for associations included population and demographic characteristics, human movement and travel history compiled using the Chi-square test. During the study period, transmission due to outside and imported cases showed a decline. However, reconciliation showed more demographic cases for preschool, school children and elderly women also known as dependent groups. Outside transmission was associated with young adults and adult groups, male, and non-Thai-migrants. In the study, the population was divided into outside, imported transmission and also indoor transmission species groups. The number of imported cases remained consistent all the time. Therefore, sole infection data along with travel date and clinical history can be used to know the origin of cases and detect epidemiological linkage of cases, which would enhance efficacy and use of limited cases. Sole infection data could be used to tailor specific interventions.
Maylis Douine (Cayenne Hospital, French Guiana) presented the results of an operational research study in the Amazon on self-diagnosis and self-treatment for malaria known as the Malakit Project. French Guiana is in the Amazon Guiana shield of South America where the soil is rich in gold, hence attracting a lot of miners with high malaria prevalence. The main objective of the study was to understand and increase, the use of early and adaptive treatment with good compliance, with a secondary objective to improve knowledge of practices and decrease malaria prevalence. The distribution and training of Malakit use were done by facilitators from the target population for 2 years. The study employed cross-sectional and qualitative survey data collection for participants’ opinions on the use of the kit. Results indicated that more than 70% of people correctly used the kit. Testing before treatment certification increased and the proportion of Plasmodium falciparum decreased before and after intervention compared with PCR prevalence of Pf Impact evaluation on malaria epidemiology. Douine concluded that the impact on malaria incidence estimates that Malakit prevented 46% of imported cases.
May Me Thet (Population services international, Myanmar) presentation was about the role of rural private sector providers in malaria surveillance and case management during the COVID-19 pandemic in Myanmar. Myanmar has 3 types of health providers named: health quality medical doctors channeled practitioners based in urban areas, trained informal providers called private armlets, and community volunteers, working in rural areas. During the COVID19 pandemic, service provisions were affected in both the private and public sectors. The study evaluated the performance and quality of the 3 service providers of service before and after the pandemic. Data analyzed were generated using a routine management information system database that incorporates clinic data, private outlets and volunteers. Audit testing and positive case findings, as well as service quality scores, were used to compare service providers. Results highlighted that performance in medical doctors audit testing per month decreased while private outlets testing increased, and that service scores were similar among the 3 service providers which were statistically significant.
Will Stone (London School of Hygiene and Tropical Medicine, England) presented on gametocyte persistence, infectivity and associations with histidine-rich protein 2 (HRP-2) levels after pyronaridine-artesunate and dihydroartemisinin-piperaquine with and without single-low dose primaquine, assessed using a single-blind randomized clinical trial in Ouelessebougou, Mali. The primary endpoint was within arm reduction in the proportion of mosquitoes infected by participant blood samples 48 hours post-treatment. Secondary endpoints included infectivity to mosquitoes at other time points, measures of gametocyte density and sex ratio and safety measures including the frequency of adverse events and hemoblogin concentration. Infectivity to mosquitoes was measured using direct membrane feeding assays which found infectivity stopped almost immediately in arms with PQ; 10-20% of individuals were still infectious after 21 days with ACT alone. They also tested HRP2 detectability because gametocytes continue to circulate in the blood for long periods after standard ACT treatment. Stone concluded that results found no significant differences in HRP2 concentration determined by Quansys ELISA between ACT treatment groups with or without primaquine and there were no differences.
Erica Berlin (Clinton Health Access Initiative – CHAI, United States of America) presented on the use of qPCR and serology to inform targeting malaria elimination strategies in low burden settings in Botswana. A Malaria Transmission Limits Survey (MTLS) was implemented in 3 districts in 2018 with the objectives of determining whether malaria transmission was present and at what intensity, to determine the limits of malaria transmission by detecting current and past infections, and to describe potential factors associated with malaria transmission by administering a questionnaire. Populated blocks of 5×5 km were identified that contained at least 10 structures; they were prioritised according to high risk or high uncertainty as to risk based on incidence estimates. Based on the survey, estimated qPCR-prevalence of malaria in the peak season was <0.1% for all 3 districts. Overall, 20% of adults surveyed were seropositive; lower seropositivity in participants under 18 years suggest that transmission has decreased markedly over the past 2 decades. The majority of people with high antibody response had not travelled in the past month, but the small number that did, travelled within Botswana, indicating local transmission. In conclusion, Berlin said that transmission appears to be declining over time, there is low risk of importation and reintroduction, and serology and qPCR confirmed findings from the case-based surveillance system that fishermen and farmers are the most exposed.
Symposium #65: Malaria: Drug Treatment, Resistance and Clinical Trials
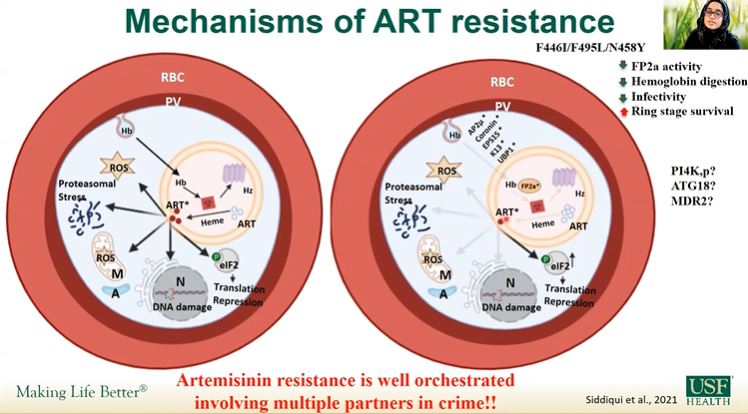
Faiza Siddiqui (University of South Florida, United States of America) discussed various ways to deeply explore molecular markers involved in artemisinin resistance with a great focus on PfK13. Siddiqui and team used a green fluorescent protein to study the expression and localization of PfK13 protein in asexual and sexual stages. Some of the K13 mutations tested show lower fitness and higher ring stage survival under drug pressure They used a new antibody against PfK13 to show that the PfK13 protein is expressed ubiquitously in both asexual erythrocytic stages and gametocytes and is localized in punctate structures, partially overlapping an endoplasmic reticulum marker. She partially concluded that some parasites showing resistance phenotypes lack K13 mutations. Siddiqui highlighted the need to identify additional markers of resistance. Artemisinin resistance selection using Dd2 strain and genome sequencing has identified SNPs in other genes (e.g. PI4K, ATG18 or MDR2). Further studies determining all contributors towards resistance are needed.
Melissa Rosenthal (University of Nebraska Medical Center, United States of America) started her presentation by establishing a relation between Plasmodium falciparum and various peroxides including artemisinin, arthemether and artesunate. She talked about various protein damage caused by artemisinin in parasites resulting in accumulation of ubiquitinated proteins which are then degraded by the parasite proteasome. She presented both non-selective proteasome inhibitors and Plasmodium-specific proteasome inhibitors. Then, Rosenthal hypothesized that the proteasome is critical for parasite ART-response and mutations decreasing proteasome catalytic activity reduce the ability of parasites to recover following ART-induced protein damage. Proteasome mutants exhibit decreased β2 and β5 catalytic activity in response to dihydroartemisinin (DHA). Rosenthal’s team found that β5 A20S does not compromise peroxide potency and increases synergy in some peroxide combinations. On the other hand, β2 proteasome mutants display increased sensitivity to DHA and the related endoperoxide OZ439. She also reported an increase in sensitivity observed not only at early ring stages where ART resistance is classically observed but also at trophozoite stages and in asynchronous cultures. The sensitivity throughout the intraerythrocytic development is likely due to the necessity of the parasite proteasome throughout its lifecycle. She highlighted the importance of the parasite proteasome in response to endoperoxides.
Recently, resistance to the antimalarial artemisinin has been reported in Uganda, posing the threat of the emergence and spread of artemisinin resistance in Africa. Jean Moïse Tanga Kabore (Health Action Research Group – GRAS, Burkina Faso) presented a pilot study that aims at assessing the feasibility of a strategy deploying simultaneously three artemisinin-based combination therapies (ACTs) at health facility (HF) level for the management of uncomplicated malaria in Burkina Faso. Strategy was aimed at delaying the spread of resistance to ACT treatment. The study population was segmented in 3 groups receiving at HF-level either pyronaridine-artesunate (patients under 5 years), dihydroartemisin-piperaquine (5 years and above), or artemether-lumefantrine (AL) (pregnant women). The community case management of malaria continued with no change using AL. Tanga showed that over the 12 months of the study, 182,247 and 4,955 malaria cases were seen at HF and community level respectively and treated with ACTs. No serious adverse drug reaction was reported. The compliance with the multiple first-line therapies (MFT) protocol guidelines was adequate for three quarters of health workers (HWs) and there was a good management of ACT stocks over the study period. He concluded that the implementation of an MFT strategy in Burkina Faso is feasible and well accepted by the HWs, and that a scale-up is conceivable.
Mackenzie Sievert (Eck Institute for Global Health, United States of America) mainly discusses the improvement of the ring stage survival assay (RSA) serving artemisinin resistance measurement. He presented different assay modifications that increase efficiency and/or precision of this assay. Sievert and team adjusted culture volumes, synchronization and used improved equipment (flow cytometer, 96 well plate and qPCR) then developed a modified RSA. This tool improved correlation with patient clearance half-life and significantly reduced experimental noise and labor intensiveness. This also allowed the higher throughput needed to quickly phenotype large numbers of parasites in less time. He conducted several experiments; resistance was inferred at 120hours as a differential between treated and untreated parasites then combined with an additional 192h post-treatment sample to generate a recovery profile. He reported that recovery expands their view of the drug response phenotype. This study reveals that the growth, resistance and recovery assay combines more detailed fitness phenotypes, greater correlation to clinical phenotype and additional drug response phenotype to differentiate sensitive parasites. This serves as a novel and complementary phenotype to resistance that quantifies a parasite’s ability to tolerate drug exposure, a hallmark of parasite response to ART.
M5717 is an antimalarial compound acting on all life stages of the malaria parasite, and inhibiting the Plasmodium falciparum elongation factor 2 (PfeEF2). Johan van der Plas (Centre for Human Drug Research, the Netherlands), presented the results of a Phase Ib, randomized, double blind, sequential, adaptive dose-finding study to assess M5717 chemoprophylactic activity in healthy male and female volunteers inoculated with P. falciparum sporozoites. The initial cohorts followed a dose de-escalation pattern and the effect of single doses ranging from 200 to 30 mg was evaluated. The study showed that M5717 is well tolerated, and that there were no potential risks or safety concerns whatever the dose compared to existing clinical data. The safety profile did not indicate any treatment of emergent adverse events (TEAE) leading to death or discontinuation, and no serious IMP-related TEAEs. Van der Plas then presented the proof of chemoprophylactic activity of M5717, showing that a single dose of ≥ 100 mg provided 100% protection in liver-stage controlled human malaria infections. There was no evident difference in protection rate in early and late liver-stage models. Altogether, the results of the study warrant further development of M5717 as part of a chemoprevention combination for malaria and can guide rational dose selection in prophylactic clinical trials.
Tafenoquine (TQ) is a long-acting 8-aminoquinoline that has activity against hepatic stage schizonts, and Plasmodium vivax hypnozoites, as well as less well-characterised activity against blood stage parasites and gametocytes. Bridget Barber (QIMR Berghofer Medical Research Institute, Australia) presented a 2-part study investigating the effective dose of TQ to clear blood-stage P. falciparum parasitaemia (Part 1), and to prevent transmission of P. falciparum to mosquitoes (Part 2). Part 1 results showed that low dose (300 mg) of TQ was not efficacious at clearing asexual parasitaemia in healthy volunteers experimentally infected with blood-stage P. falciparum. The development of a PK/PD model is underway and preliminary results show that none of the participants treated with TQ 200 mg achieved complete parasite clearance, while the model shows efficacious dose prediction for participants treated with 300 mg TQ higher dose will be needed (6 log kill: 520 mg; 9 log kill: 850 mg). In the second part of the study, she showed that 50 mg TQ reduced transmission intensity by 75% by day 7, and that there was a good correlation between oocyst and sporozoite positivity rate. Further studies are underway to address limitations and remaining questions, such as how results translate to field settings, or the duration of the transmission blocking effect.
Artemisinin-combination based therapies (ACTs) are threatened by the emergence and spread of Plasmodium falciparum parasites less susceptible to artemisinin derivatives and their partner drugs. Thierry Masserey‘s (Swiss Tropical and Public Health Institute – Swiss TPH, Switzerland) research work consists of identifying the key drivers of establishment and spread of malaria parasites. He presented the results obtained using an adapted stochastic individual-based model of malaria epidemiology and transmission dynamics that allows the systematic quantification of the influence of biological, transmission settings, health systems, and pharmacokinetics/ pharmacodynamics factors on the establishment and spread of drug-resistant parasites. The spread of resistance to artemisinin extends because parasite exposure to artemisinin derivatives when used in monotherapy and delays the evolution of resistance to the partner drugs when used in combination therapies. When used in monotherapy, the spread of resistance to partner drugs reduces the selection pressure caused by the period of low drug concentration. Low transmission intensity favours the evolution of drug-resistance. Masserey concluded that the resistance to the partner drug has an essential role in promoting evolution of resistance to artemisinin. These results could have implications for delaying resistance to artemisinin by ensuring adherence to treatments and that no resistance to the partner drug exists in the target population, and for informing future artemisinin therapies using additional long-acting drugs as partners to minimize the selection window.
Symposium #71: Challenges in Malaria Diagnosis
Jessica McCaffery (Centers for Disease Control and Prevention, United States of America) presented a study titled, ‘Use of a Novel Plasmodium vivax Chimeric Protein for Malaria Serosurveillance in Multi-species Endemic Countries Nearing Elimination’. McCaffery presented results from a proof of concept study that was conducted in USA travelers returning from malaria-endemic countries with PCR confirmed parasitemia. They used chimeric PvMSP1 (cPvMSP1) to capture IgG and found that cPvMP1 was recognized by the majority of these PCR positive travelers regardless of species causing infection. After confirming that cPvMSP1 can capture malaria-specific IgG in infected travelers more broadly and with higher signal than recombinant PvMSP1 (rPvMSP1), they conducted a seroprevalence study in two malaria endemic areas nearing elimination in Ethiopia and Costa Rica. Results showed that seroconversion rates reflected malaria transmission history of the study sites. Ethiopia’s seroconversion model suggested cPvMSP1 may detect both P. falciparum (Pf) and P. vivax (Pv) infections combined or showed increased sensitivity of cPvMSP1 over rPvMSP1, while in Costa Rica’s seroconversion was detected earlier for cPvMSP1 than rPvMSP1. McCaffery described the benefits of engineered antigens by highlighting its ability to be tailored to determine pan-Plasmodium exposure or for species-specific detection as it can be designed to include highly recognized epitopes resulting in increased sensitivity and accuracy of detection. She concluded that multiplex assays offer a way to estimate malaria transmission, and using engineered antigens alongside established recombinant antigens in multiplex seroprevalence studies can help to identify high-transmission areas.
Dean Sayre (Centers for Disease Control and Prevention, United States of America) pointed out that Cambodia had the second-highest number of malaria cases in GMS in 2020. Although intense national efforts have helped in reducing malaria cases in the past few years, Pv cases are still accounting for most of the cases in Cambodia. The country is aiming to eliminate Pf by 2023 and Pv by 2025. Considering the unique ability of Pv to become dormant in the liver stage, elimination efforts require intervention specifically for tackling the hypnozoites. Although primaquine and tafenoquine can eliminate hypnozoites, these drugs can cause destruction of red blood cells, or hemolytic anemia, in individuals with inadequate amounts of the enzyme glucose-6-phosphate dehydrogenase (G6PD) deficiency, which can be lethal in some cases. Sayre presented results from clustered, cross-sectional surveys of adults from the Kampong Speu province, that evaluated the performance of the quantitative point-of-care (POC) G6PD activity assay STANDARD™ G6PD (SD Biosensor, Republic of Korea). The study consisted of two phases, a community phase and a health-facility phase. The POC, which uses capillary blood, was compared against the gold standard laboratory method (spectrophotometry) that used venous blood. In the community phase, the POC assay was 93% (85–100%) sensitive for detecting individuals with ≤ 30% median G6PD activity (negative predictive value, NPV = 99% (98—100%)). Using ≤ 70% median G6PD activity as the cut-off, POC sensitivity was 65% (53-78%), with NPV = 88% (81—94%)). Results from the community phase resulted in modifications in specimen transportation procedures for the health-facility phase. Data for this phase is preliminary but suggests that the POC assay can accurately identify those at the highest risk of primaquine-induced hemolytic anemia.
Han Zhang (Harvard University, United States of America) presented a study on the impact of malaria rapid diagnostic tests scale-up on antibiotic use in 21 sub-Saharan African countries. Here, they constructed a dataset with related individual-level information from 3 data sources (demographic and health surveys, the Malaria Indicator surveys, and the Multiple Indicator cluster surveys) and explored the variation in mRDT distribution from a major donor – U.S President’s Malaria Initiative (PMI) over a 10-year period (2009-2019). Results showed that PMI total mRDT distribution across study countries was about 496.7 million, with huge variation across countries and a dramatic scale-up over the period. This study further determined a correlation between PMI mRDT distribution scale-up and increased testing uptake for children <5 years with fever. She highlighted that mRDT scale-up had a heterogeneous impact on antibiotic use by malaria parasite prevalence and by place of care. Zhang concluded that work is ongoing to explore the health implications resulting from the change in antibiotic use as well as improvement measures on regional-level mRDT distribution.
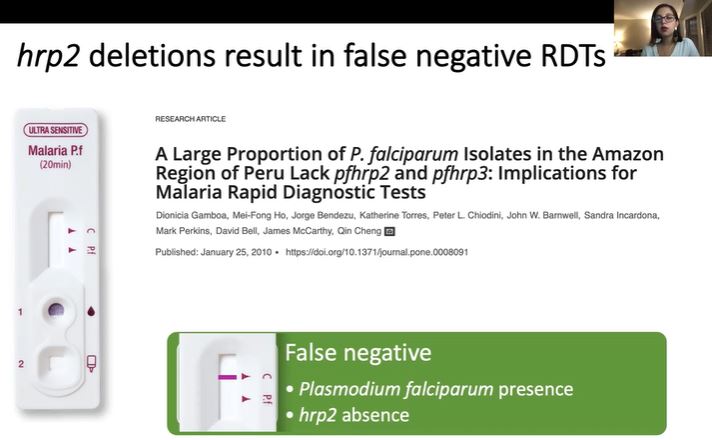
Rapid diagnostic tests (RDT) are easy-to-read devices with field applications in malaria. Common RDTs target the Histidine-Rich Protein 2 (hrp2) antigen, but many countries report parasites with hpr2/hrp3 gene deletions, undetectable by these RDTs. Claudia Vera-Arias (University of Notre Dame, United States of America) used digital droplet PCR (ddPCR) for the molecular surveillance of hrp2/hrp3 deletions to circumvent the difficulties of nested PCR (nPCR). A novel dPCR was optimized on 2 systems (BioRad QX200 and Qiagen Qiacuity). The assay was compared to nPCR using triplicates of 248 samples of asymptomatic infections from western Kenya, nPCR gave 12.3% false-negative results when compared to ddPCR. Also, mixtures of lab strains with the hrp2 deletions (Dd2) and wild-type (3D7) were used to test the effect of polyclonal infections. ddPCR reliably detected mixed infections if mutated parasites were >40%. The new ddPCR assay was used to type samples from Kenya (241), Zanzibar (Tanzania) (91), Ghana (223), Ecuador (41), Brazil (187), and southwestern Ethiopia (47). No deletions were observed in Kenya, Ghana, and Tanzania; in Ecuador, no hrp2 deletions were observed, but 53.7% of samples carried hrp3 deletions. In Ethiopia 2.1% carried a hrp2 deletion, and 74.5% hrp3 deletions (2.1% hrp2/hrp3 double deletion) and, in Brazil, 46.5% of samples carried hrp2 deletions, and 62% hrp3 deletions (46% hrp2/hrp3 double deletions).
Near-infrared spectroscopy (NIRS) has been previously applied in mosquito surveillance to identify and characterize types of malaria infections. Maggy Sikulu-Lord (The University of Queensland, Australia) presented the results on the evaluation of a rapid, reagent-free, and non-invasive malaria detection tool based on NIRS. Using a mouse malaria model, infrared light was shined briefly on the ears, feet, groin, and tail of mice with and without Plasmodium berghei malaria infection at multiple time points to collect reflected spectral signatures. Mice were divided in two groups and were scanned before (0 hrs) and after (24, 48, and 72 hrs) infection. Machine learning was then applied to differentiate infected from uninfected mice. Positive predictive rate (PPR) and negative predictive rate (NPR) of NIRS were 90% and 100% when parasitemia levels were ≥2%, being consistent with microscopy results. Using the same principle, a handheld NIR spectrometer was used to scan arms, fingers, and ears of 12 human volunteers who were either uninfected or infected with P. falciparum or P. vivax. The model built by machine learning detected infections with 100% sensitivity and 83% specificity. Sikulu-Lord emphasized that, although the results are promising, more data from the field will be required to verify the diagnostic capacity of NIRS.
Wataru Kagaya (Osaka City University, Japan) discussed a study conducted in 2020 at the Homa Bay County referral hospital in western Kenya. The goals of the study were to 1) apply XN-31p for mass malaria surveillance in the field; 2) test its applicability to capillary blood samples; and 3) evaluate the effect of sample storage time and temperature on results stability. Capillary and venous blood samples collected from 169 outpatients in which clinical malaria was suspected were tested with XN-31p, microscopy, RDT, and PCR. The sensitivity and specificity of XN-31p with capillary blood samples (using PCR as the gold standard) were 85.7% and 100%, respectively, with results being comparable to RDT and microscopy. Results with the XN-31p maintained stability in samples assayed 24 hours post-collection, and capillary and venous blood samples showed concordance. Kayaga added that an advantage of XN-31p is that it is automated, so there is no need for special training to use it. As the next step, his team intends to assess the performance of XN-31p against asymptomatic or submicroscopic infections and for the diagnosis of Pf and non-Pf mixed infections.
Retno Utami (Eijkman Institute of Molecular Biology, Indonesia) presented a study entitled ‘Identifying future Plasmodium vivax relapses with serological markers of exposure in a returning Indonesian soldier cohort’. She explained that Pv is endemic in the Indonesian archipelago, where the proportion of Pf to Pv cases is approximately 1:1. Blood samples were collected from a cohort of 294 Indonesian soldiers at high risk of acquiring malaria infections who were free of acute Pv infection by microscopy after returning to the non-malarious area of East Java after a tour-of-duty in the moderately malaria-endemic area region of Papua. Enrolled participants were followed by active and passive surveillance for the first 6 months after returning to East Java. Serology for 19 exposure markers was conducted in all enrollment and follow-up samples by Luminex. Using random forest classification, a panel of eight serological exposure markers (SEMs) showed 75% sensitivity and 93% specificity in identifying individuals with hypnozoite and those at risk of future relapse infections during the 6-month observational period. Thus, SEMs successfully identified malaria-exposed but uninfected individuals at risk for subsequent relapse infections.
This report is brought to you by the MESA Correspondents. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri (Lindsley F. Kimball Research Institute, New York Blood Center, USA). This report is cross-posted on the MESA website and on MalariaWorld.
Published: 22/11/2021
This report is brought to you by the MESA Correspondents Edima Ottoho, Tope Kayode, Franklin Tembongshu Formilack, Lucy W. Mwangi, Vita Mithi, Ana Alonso, Faith Hungwe, Olajoju Temidayo Soniran, Isabelle Delrieu, Patricia Doumbe Belisse, and Carlos A. Fernández Miñope. Senior editorial support has been facilitated by the Organizers and Co-Chairs of the symposia and Divya Beri.
THEMES: Basic Science | Epidemiology | Health Systems
Related Resources